Introduction: The True Source of Gout Pain
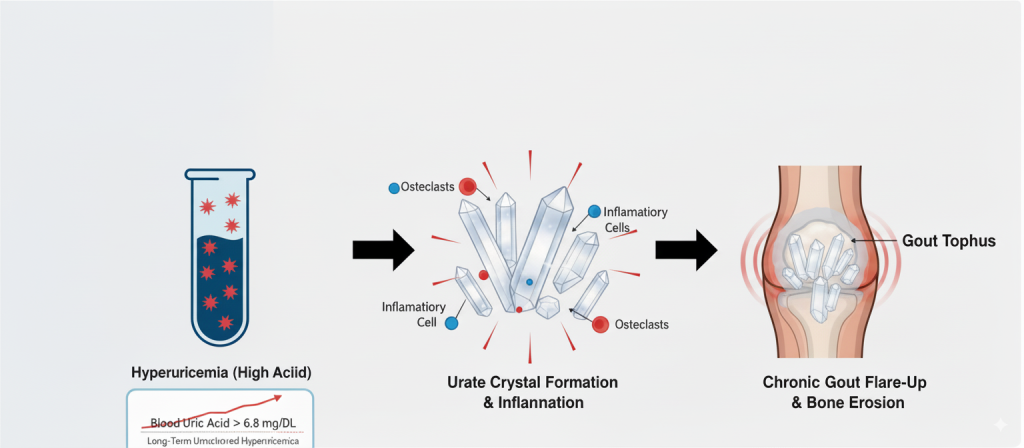
For anyone who has experienced gout, the first word that comes to mind is pain. But the true source of this agony is often the silent formation of what are known as “tophi” in your hands, feet, and other joints.
Gout tophi are the direct result of long-term, uncontrolled hyperuricemia (high uric acid). When the concentration of uric acid in the blood consistently exceeds its saturation point (around 6.8 mg/dL), it begins to crystallize. These deposits are not inert; they are biologically active granulomas that actively promote inflammation and bone erosion by recruiting inflammatory cells and osteoclasts. As these crystals accumulate, the body’s immune system attacks them, triggering the intensely painful flare-ups characteristic of gout. After repeated attacks, the urate crystals become encapsulated by fibrous tissue, forming hard, chalky nodules—the tophus.
Tophi are more than a cosmetic issue; they are a definitive sign that your body’s uric acid metabolism is severely dysfunctional. Their presence leads to chronic pain, joint destruction, and limited mobility. The overlying skin can rupture, risking severe infection that, in worst-case scenarios, can lead to amputation.
Current Treatment Methods and Their Limitations
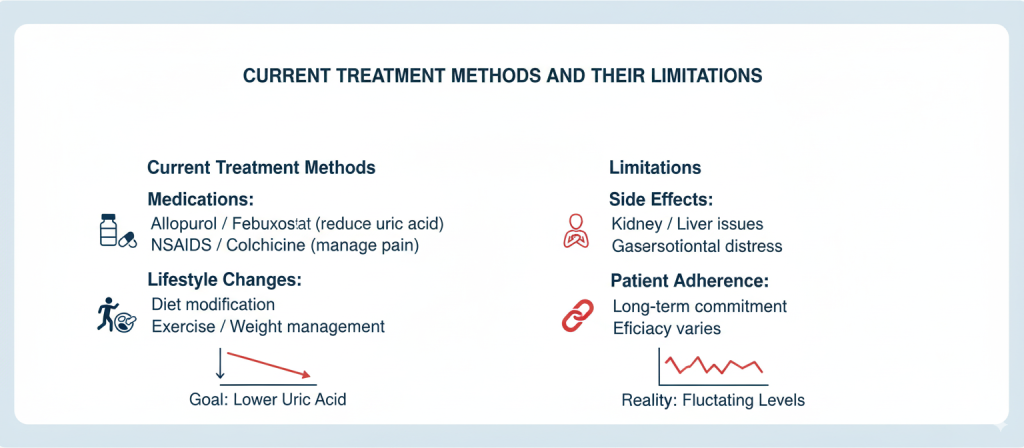
Medicine offers several approaches to dealing with tophi, but each comes with its own set of limitations.
1. Surgical Removal: An Immediate but Superficial Fix
- Method: For tophi that cause severe deformity, nerve compression, or recurrent infections, surgical excision can provide immediate relief.
- Limitations: Surgery is invasive and carries risks. More importantly, it is not a cure. Clinical consensus confirms that without aggressive post-operative urate-lowering therapy, recurrence of tophi is almost inevitable because the underlying metabolic issue remains unaddressed.
2. Urate-Lowering Therapy (ULT): The Foundation, but a Slow-Acting One
- Method: The cornerstone of tophi management is lowering uric acid with medication. The goal is to create an “unsaturated” environment where crystals can dissolve. The American College of Rheumatology (ACR) recommends maintaining a serum uric acid level below 6 mg/dL, and for patients with tophi, a more aggressive target of <5 mg/dL (300 μmol/L) is strongly recommended to promote dissolution.
- Limitations: This process is incredibly slow. Studies have shown that while effective, dissolving large tophi with medication can take many months to several years. The rate of resolution is directly proportional to how consistently the low uric acid target is maintained. Any interruption in medication can cause urate levels to spike, undoing years of progress.
3. Physical Therapy: An Auxiliary Method with Limited Evidence
- Method: Emerging therapies like extracorporeal shock wave therapy (ESWT) and ultrasound are being explored to help break down tophi.
- Limitations: Currently, robust evidence from large-scale clinical trials is lacking. These methods are considered experimental, and their role in standard clinical practice remains unproven and is not included in major treatment guidelines.
The Root of the Problem: Lowering Uric Acid is the Only True Solution
All effective treatments for gout tophi are built on one fundamental principle: sustained and effective reduction of blood uric acid levels.
Think of it like a flooded room. The faucet (your body’s uric acid production) is leaking, and the water on the floor (the tophi) is getting deeper.
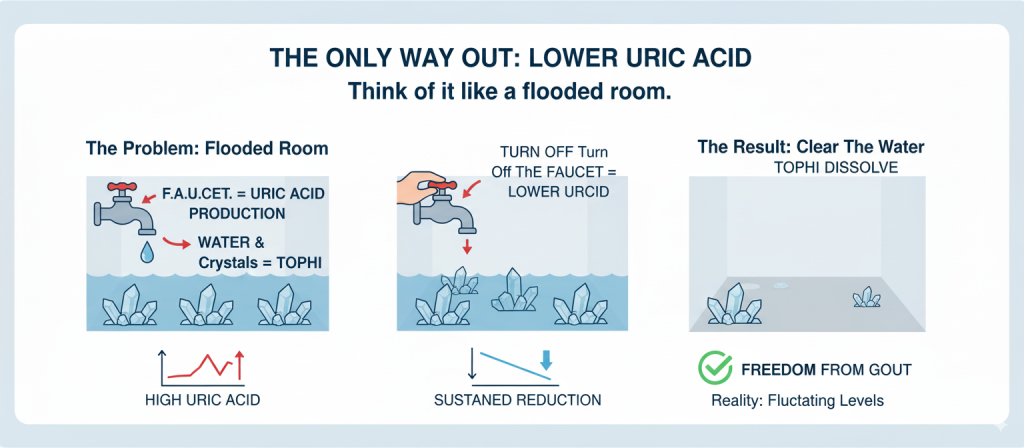
- Surgery is like mopping up the water.
- Conventional drugs are like turning the faucet down and slowly clearing the drain.
If you don’t fix the leaky faucet at its source (i.e., correcting the uncontrolled uric acid metabolism), the room will inevitably flood again. Therefore, the treatment of gout tophi must return to its origin: long-term, regulated reduction of uric acid to address the root metabolic issue.
BISPIT Gold 3310-S: A Multi-Pronged Approach to Gout Management

BISPIT Gold 3310-S is a scientifically formulated blend of potent herbal extracts designed to work synergistically. It addresses the problem from three key dimensions:
- Lowering Uric Acid: To stop new crystals from forming.
- Dissolving Crystals: To address the immediate problem of existing tophi.
- Controlling Metabolism: To tackle the root cause and prevent recurrence.
By helping to stabilize blood uric acid below the 300 μmol/L (5 mg/dL) threshold, it supports the body’s shift from a “supersaturated” to an “unsaturated” state, allowing urate crystals to dissolve. The 3310-S formula has also obtained an NDC number in the United States, a mark of quality and safety.
Unlike the “war of attrition” fought with traditional drugs, BISPIT 3310-S is designed to address the “efficiency issue.” It is formulated to target and dissolve crystals, and includes ingredients like glucosamine and Lysimachia christinae extract to help mitigate the discomfort that can occur during the dissolution process, with noticeable changes often felt within the first bottle.
For best results, this should be combined with lifestyle interventions proven to aid in gout management: a low-purine diet, reducing alcohol, staying well-hydrated (over 3000ml daily), and managing weight. This multi-faceted approach helps halt the formation and progression of tophi at their source.
Conclusion: No Shortcuts to a Tophus-Free Life
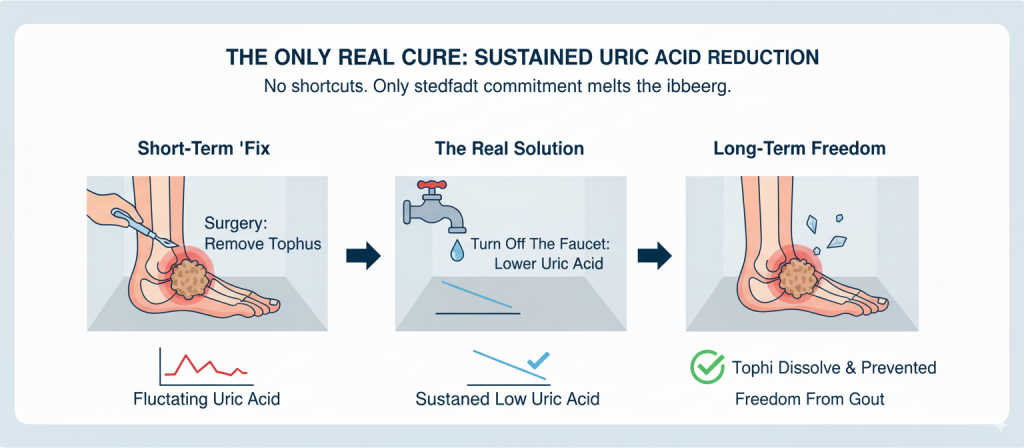
There are no shortcuts in the treatment of gout tophi. Surgery can solve an immediate crisis, but only a steadfast commitment to maintaining low, stable uric acid levels can truly melt the iceberg and clear the source. This is the only evidence-based way to make tophi a thing of the past and prevent their devastating return.
Data Sources:
Dalbeth, N., & Haskard, D. O. (2005). Mechanisms of inflammation in gout. Rheumatology, 44(9), 1090-1096. This paper details how urate crystals trigger an intense inflammatory response, leading to the formation of the tophus as a chronic granulomatous process.
Richette, P., & Bardin, T. (2010). Gout. The Lancet, 375(9711), 318-328. A comprehensive review covering the pathophysiology of gout, including the severe clinical consequences of untreated tophi like joint destruction and skin ulceration.
Lee, S. S., & Lee, D. H., et al. (2018). Factors associated with the recurrence of tophi after surgical excision in patients with gout. The Journal of Foot & Ankle Surgery, 57(3), 532-536. This study highlights the high recurrence rate of tophi post-surgery if serum uric acid levels are not adequately controlled.
FitzGerald, J. D., Dalbeth, N., et al. (2020). 2020 American College of Rheumatology Guideline for the Management of Gout. Arthritis & Rheumatology, 72(6), 879-895. These official guidelines establish the standard of care, including the serum urate targets of <6 mg/dL for all gout patients and a stricter target of <5 mg/dL for those with tophi.
Perez-Ruiz, F., Calvo, E., et al. (2002). The course of tophi in patients with chronic tophaceous gout after achieving a serum urate level below 6 mg/dl. Arthritis & Rheumatology, 46(12), 3267-3272. A key study demonstrating that tophi do resolve with urate-lowering therapy, but the process is slow and directly dependent on maintaining low serum urate levels.